

Employer-Sponsored Insurance
Why it is unnecessary and harmful

America’s health insurance system is primarily run through employers. Federal law gives money spent by an employer or contributed by the employee tax exempt status, when it is used to purchase health insurance. Today it is practically the only source of pooled health insurance available, with 90% of private health plans being through an employer (Employee Benefit Research Group, 2000), and with employers paying for about 20% of American healthcare costs through direct contributions. 61% of non-elderly population receives employee sponsored health insurance. On average, each employer pays 83% of the cost of premiums, and the employee covers the other 17%. There is no cap on the amount of money which may be paid in premiums, and the program disproportionately benefits the middle class, although as a share of income it becomes irrelevant for the wealthiest.
It is a very bad system. It increases healthcare costs, and increases what we consume in healthcare relative to what we would otherwise want, thereby decreasing the utility we get from our dollars. While there are serious arguments that the pooling that employers create is better than doing nothing at all, it is far worse than either a nationalized healthcare system, or a simple mandate that everyone purchase health insurance. I am against it, and believe we would be better off either with a total repeal of the tax exemptions for employer sponsored insurance and for self employed individuals, or, if that is politically impracticable, the amount that can be made tax exempt should be capped. (What was referred to as the “Cadillac Tax”, when such a cap was included in the Affordable Care Act.)
The program has been described as an historical accident. Health benefits first became tax exempt in 1915, but they did not become prominent until the Second World War, when employers faced strict controls on wages. Looking for a way around the price controls, companies offered more generous health insurance plans. (Carrol, NYT, “The Real Reason the US …, 2017) After the war, unions began to push for including more health insurance as part of benefits, as due to economies of scale and pooling benefits, they were easier to achieve than wages alone, (in addition to the more cynical motive, more common today, that pushing for health insurance instead of wages disproportionately benefits full members of the union above part time workers or workers who just started.) Enrollment in employer sponsored health insurance plans increased from under 20 million in 1940, to over 120 million people by 1960. (Sourcebook of Health Insurance Data, 1965.
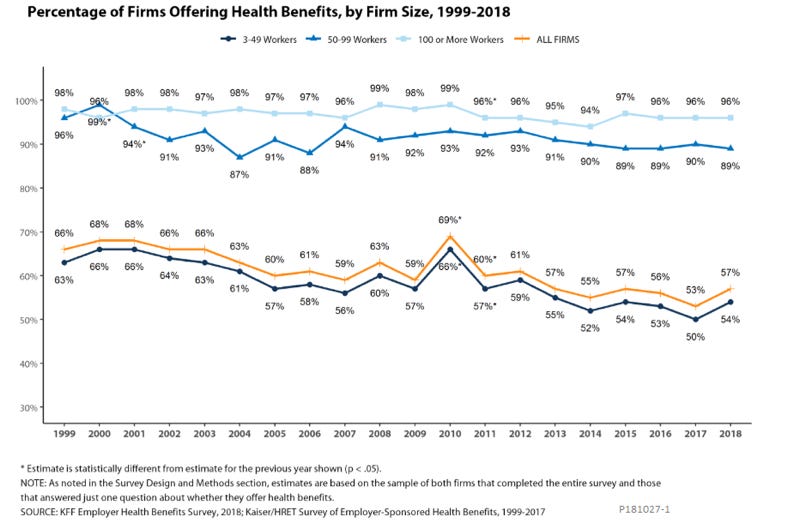
Large employers, defined as those with greater than 100 employees, almost universally offer health insurance benefits, while small firms (which are much more numerous, although this can be misleading - while 98.1% of firms employ fewer than 100 people, firms with greater than 100 people employ 77.6% of workers.) are still more likely than not to offer health insurance plans.
The Clinton health insurance plan, proposed in 1993, would have built a universal healthcare system based on employer mandates. However, the bill failed due to conservative opposition. In 2010, the Affordable Care Act, while not getting rid of employer healthcare’s tax exempt status, simply put the insurance mandate on all people, and did not need to go through employers.
The principal argument in favor of employer sponsored health insurance is that it acts as a pooling mechanism. (Mulligan, 2021, Gruber, 2010) A pooling mechanism is a way to get a sample of people with a random, but predictable, need for healthcare. This avoids the problem of adverse selection. In an unregulated market, what could happen is that people who know they are quite healthy, and thus will have less need for health insurance, opt out of insurance entirely. With these healthy people having left the market, rates must go up for the insurance company to still make a profit, making another rung of mostly healthy people leave, and so on. Insurance being through employers alleviates this - it creates a pool of workers, more or less randomly selected - and while adverse selection does not go away entirely (people are still able to select jobs based, to some degree, on what sort of healthcare coverage they can get, and people with severe conditions requiring expensive treatment may be denied a job (especially by small businesses)) it is lessened enough that the market can function. The fact that health insurance is bought as a group also reduces administrative costs. As Buechmuller and Monheit put it in “Employer-Sponsored Health Insurance and the Promise of Health Insurance Reform, “...because important administrative costs vary with the number of contracts, rather than the number of individuals covered by a contract, there are substantial economies of scale associated with purchasing insurance through a group… the administrative load for ESI is roughly half that for individually purchased policies: 15 to 20 percent compared to 30 to 40 percent (Swartz 2006).”
Another argument is that health insurance plans sponsored by an employer have the ability to demand bulk discounts. By changing which doctors, hospitals, or other providers are part of their network, they can make their demand for healthcare extremely elastic. Casey B. Mulligan’s 2021 paper, “The Value of Employer-Sponsored Health Insurance”, estimates that beneficiaries paid $100 billion less than comparable individuals in the ordinary private markets paid.
Another argument in favor is that running health insurance through employers allows people to specialize in choosing healthcare plans. People are rather bad at choosing healthcare on their own - we are dizzied by choice, do not have a sound grasp on risks, and are easily suckered. Abaluck and Gruber, in “Choice Inconsistencies among the Elderly”, found that if elderly purchasers of Medicare Part D plans had purchased rationally, welfare would have been 27% higher. Employers can hire a few people to make better choices on our behalf.
A much less serious argument, but one which is believed by, if you will trust my estimation, a majority of Americans, is that employer sponsored health insurance raises pay by making the employers pay for it. It does slightly, but extremely inefficiently. Were it our aim, we’d be vastly better off just mailing people checks. Gruber and Krueger, in “The Incidence of Mandated Employer-Provided Insurance”, find that somewhere between 56% and 85% of health benefits dictated by mandates are passed on to employees. The benefits in healthcare transferred to employees via a tax deduction without a corresponding drop in wages is much harder to measure, because we have not had exogenous variation in tax exempt status of the kind which would be needed to run a study, but theory would suggest that it be much closer to 100%. After all, the program is voluntary, not an imposition as a mandate would be, and we’ve no reason to believe employers would increase wages anymore than they needed to to attract workers. Any increase in real compensation would have to be because of efficiencies of scale in providing healthcare.
These arguments may seem convincing on their face. However, they are all poorly reasoned assertions that fail to take into account what people would actually do without the distortion that the tax deduction causes. People are perfectly capable of forming groups on their own to save on costs - they do not need to be poked and prodded into doing so. Moreover, while we lack the sample to predict what a complete repeal of employer sponsored health insurance would be, the empirical evidence which we do have supports this assessment. Jonathan Gruber writes in “The Tax Exclusion for Employer-Sponsored Health Insurance”, 2010, “The first [concern] is how large an effect removing the ESI exclusion would have on employer offering of insurance. Employees value employers as an insurance purchasing mechanism for several reasons, of which the exclusion is only one; there are also the benefits of group purchase, negotiating power from group size, and ease of plan choice and administration. These will still be present even if the ESI exclusion is ended. Indeed, virtually all medium size and large firms in the U.S. have offered health insurance continuously over the past thirty years, despite enormous swings in the effective tax price of health insurance. Gruber and Lettau (2004) examine the impact of tax price variation on employer provided insurance; the larger literature on this topic is reviewed in Gruber (2004). They find that medium-sized firms are only very modestly sensitive, and large firms not at all sensitive, to the tax price of ESI. They do find that small firms are price sensitive, with an elasticity of small firm offering with respect to the tax price of -0.69. Therefore, while predicting the impacts of removing the exclusion go out of sample, there is no reason to think that there will be a wholescale [sic] exit of medium and large firms from ESI.”
Let us take the pooling mechanism. If pooling through an employer produces benefits in excess of the cost needed to provide the service, then we would expect people to do it. Employers can offer health insurance, and get more bang for their buck in terms of compensation. But let us suppose that adverse selection is still a problem. Why is it that we choose to pool through employers - a way that does not benefit the unemployed, the self employed, as well as anyone who wants a different plan - when we could simply mandate that everyone buy health insurance? That way, our pool is the whole nation - no adverse selection, no nothing. A related method of pooling would simply be to nationalize healthcare.
The appeal to administrative costs is also faulty. We are expecting either companies and/or policy holders to choose to give up a lot of money in entirely unnecessary administrative fees, when employers have the capacity to do administration more efficiently. If signing up through work got you a discount, wouldn’t anyone take it? It seems to assume that people are utterly incapable of helping themselves.
The arguments of discounts, and of specialization, likewise fail to take into account how people’s behavior would change in response to changing circumstances. If organizing into groups allows people to get cheaper healthcare, there’s no reason why people won’t. People already form buyers’ clubs - are they now unable to, with $100 billion dollars at stake? Likewise with specialization in medical decisions. Many people are not good at stocks and bonds. If they themselves tried investing in the stock market, they’d lose money, which is precisely why they don’t. Instead, they hire someone to make the decisions for them. Likewise with medical care. If you don’t understand what’s going on, you can outsource your decision making to someone else, just as you do when you take a job that provides health insurance.
There is precious little in the way of benefit that it can show. Now we come to the negative effects. The federal government forgoes over $280 billion a year in tax revenue. Because the deficit must be made up with higher taxes elsewhere, this is equivalent to us spending $280 billion to subsidize a given activity. The deduction is regressive. Although it becomes irrelevant as a percentage of income for the wealthiest (Woolhandler and Himmelstein, 2016), 83% of the benefits go to the top half of the income distribution. (Gruber 2010). As with any subsidy where demand is not perfectly inelastic (and it is not - Gruber and Lettau, as cited in Gruber, 2010, found the elasticity with respect to tax price to be -0.7), we will expect people to consume more relative to what they would otherwise want to, and that is indeed what we find. I quote from Gruber 2010, “Existing evidence, particularly from the RAND Health Insurance Experiment, is clear that the optimal health insurance plan features high initial cost-sharing with protection against extreme out of pocket risk (Gruber, 2007). Yet, even in today’s high health cost environment, the vast majority of employer-insured individuals have very modest cost sharing, with a relative paucity of high deductible plans in the ESI setting. While there are several competing explanation [sic] for this “overinsurance”, a leading contender is the tax subsidy to ESI.” America has the highest healthcare costs in the world, and is not particularly healthy. Our high healthcare costs are driven by increased use of services, and of staff hired per service, not by increased prices per se (with some exceptions, primarily in patent drugs). (RandomCriticalAnalysis, “Why Conventional Wisdom on Health Care is Wrong (a primer)”), which is precisely what our model of health insurance incentivizes. Not having high co-pays or deductibles encourages the excessive use of tests, procedures, and drugs, much of which is simply not cost effective. We spend more precisely because we subsidize spending more. This should not be a surprise.

A relatively minor demerit, but still substantial is job-lock. (The best paper on this is “Health Insurance, Labor Supply, and Job Mobility: A Critical Review of the Literature”, by Jonathan Gruber and Brigitte C. Madrian, 2002, from which I am drawing most of this.) Job-lock occurs in several forms: it makes it more difficult to change jobs, it discourages retirement, and encourages secondary earners in a household to work, especially if the primary earner is self-employed, or in one of the smaller firms which does not offer health insurance.
The effect on retirement is the one with the strongest, clearest evidence for. Individuals do not want to retire, and lose their health insurance, at the very least until they become eligible for Medicare. This pushes people to work longer than they would want to otherwise. Gruber and Madrian find near universal evidence that this is happening: “Despite using a variety of estimation techniques and several different types of datasets, almost every examination of the topic has found an economically and statistically significant impact of health insurance on retirement…”. People who would be happier going into retirement are staying at work into their 60s. Again from Gruber and Madrian: “In a Gallup poll, 63% of working Americans reported that they "would delay retirement until becoming eligible for Medicare [age 65] if their employers were not going to provide health coverage" despite the fact that 50% "said they would prefer to retire early–by age 62" (Employee Benefit Research Institute, 1990).” The effect of health insurance on the behavior of secondary earners is in a similar vein. Someone who might otherwise be a stay at home parent, whose spouse does not insurance through work, may work a job just to become eligible for the tax deductions. Reason alone tells us that they would have been happier had they not had to work to get a decent plan.
Job-lock also occurs through making it a hassle to change your job. This is difficult to measure - variations in healthcare coverage may correlate with unobserved differences in working conditions, and no state has done us the decency of repealing the tax deduction to give us a study. Some studies attempt to control for differences in other job amenities - others use some variation in the conditions of the employee. The most prominent one is to compare the turnover of people whose insurance comes from a spouse, versus those whose insurance comes from the company. While there is some division in the literature as to how much the difference is, and in a couple papers, if there is a difference, the consensus is that it is substantial. Having insurance through a spouse increases the chance of job turnover by 25%. Elementary economic theory says that competition raises wages by inducing people to bid up the price of labor to its marginal value. This suggests that making it harder to change jobs lowers real wages for labor. In my view, it is an under-considered part of why income inequality has increased over time.
Employer-sponsored health insurance is bad. It subsidizes us to get things we don’t particularly want. Repealing its tax exempt status would allow us to get what we actually want, instead of what we are forced to want. Nonetheless, I despair of substantial reform ever being passed. The one serious attempt to cap benefits, in the Affordable Care Act, was delayed twice, and then repealed. Perhaps in a more enlightened age we will have a repeal. Till then, may you be fully insured against injury and illness - and never need to use it.
The list of sources is attached here. Putting it in a link like this saves on space.
https://docs.google.com/document/d/15s6Tn73afRquzga9xonVqzPt3pS78t2vXhgBgr8LsUE/edit?usp=sharing
Thank you for reading!