Kidney Donation
What we do, what we know, and why you should do it

Kidney disease is one of the most expensive diseases afflicting America. Around 500,000 Americans are currently receiving dialysis. Because all of them are, by law, covered by Medicare, we spend about $50 billion a year on patients with end stage renal disease. In 2014, Medicare spent $90,000 per dialysis patient per year. The costs of dialysis were inflated by deliberate fraud, but the costs reflect the enormous resource intensity of the process. Most people go in three days a week, four hours a day, to have their blood sucked out with large needles, washed through specialized machinery, and returned. It is expensive, unpleasant, and only somewhat effective.
It is shocking that we do this when a cure exists. With a kidney transplant, none of this is needed. The patient will live a longer, better life, without needing to spend what remains of their life in a clinic chair. It also costs much less – the spending on kidney transplant patients is about about a third of the total spending on patients undergoing dialysis.
The trouble is that there are not enough kidneys to go around. In America, as in most of the world, you cannot buy a kidney. They must be donated by a living donor, or sourced from a recently deceased individual. There is universal agreement among economists that allowing kidneys to be bought and sold, or at the very least having donation be subsidized by the government, would be far better, but people are repulsed by the thought of others selling their body.
We cannot implement the best solution, but there are ways in which we can do things better. The improvement of kidney donation is one of the most important uses of mechanism design in real life. It has saved the lives of hundreds of people already, and if it is allowed to spread around the world, it could save many more. What’s more, you can participate in this. Your actions can save lives.
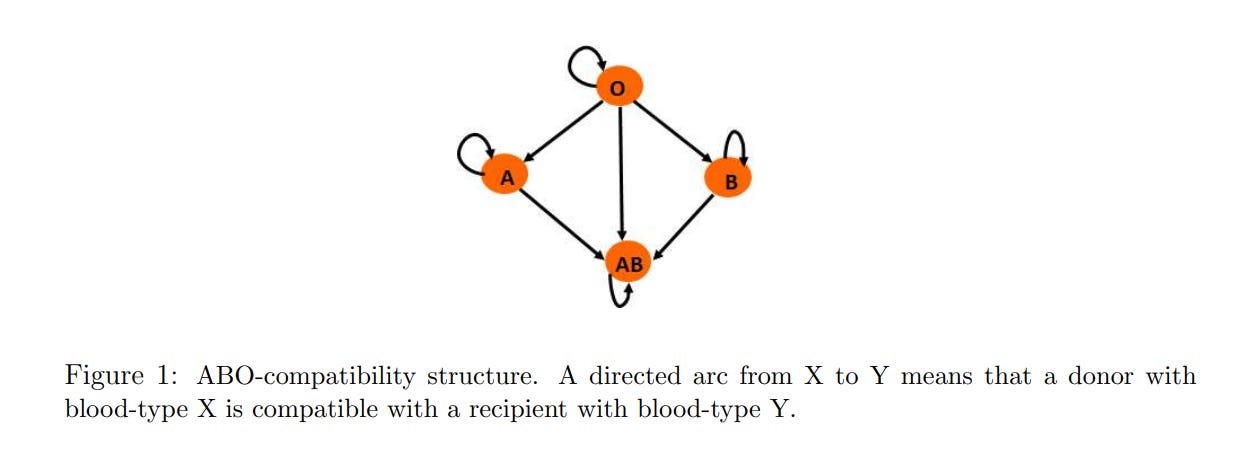
The first problem we need to overcome is that people might be altruistic only for one person, but not all kidneys are substitutable. Perhaps someone’s wife would like to donate to their husband, but she is not compatible. This might be because the blood types are incompatible, or because the tissue types cause an immune reaction in the recipient. We can imagine that there are many couples like this. We would like to find a mechanism which pairs compatible people so that everyone can end up with a kidney.
The simplest is to find bilateral trades. However, because of the many different ways in which people can be incompatible with each other, this is no guarantee of anything close to efficiency if one were restricted to only these.
What we can do instead is have an exchange. There are two basic types, a cycle and a chain. The cycle allows for us to resolve loops of people, none of whom are able to make a trade with each other, with the optimal combinations found via algorithms (covered in Ashlagi and Roth (2020)).
When agents are arriving over time, it is possible that waiting longer for agents to arrive enables better matches, at the cost of agents departing unserved because they waited too long. Akbarpour, Li, and Oveis Gharan (2020) show that waiting can be better only if the planner is able to identify who is about to leave, so that they can match them in a hurry. To my knowledge, we are reasonably able to predict how likely a person is to exit the market from their medical condition. However, in practice this concern has not led to different practices.
The drawback of the cycle is the need to do everything simultaneously. The law does not allow people to sign binding contracts to donate kidneys, and so we cannot guarantee that someone will not pull out after their recipient has received a kidney, but before they donate. It is costly to have the capacity to do many simultaneous surgeries. The size of the cycles is in practice capped at three for this reason (eight operating rooms and eight surgical teams in one hospital would be quite a lot). Thankfully, the efficiency losses are negligible when one is only concerned about blood types, although they become worse when we are more concerned about tissue type. In addition, if any part of the cycle vetoes their donor because they believe they could get a higher quality one, the whole cycle is broken and we need to make another set of offers.
This is where a chain of donors comes in. If you have someone who is donating without expecting anything in return, then you can get a chain of arbitrary length which requires nobody to donate before their recipient gets a kidney, and ends only when someone reneges (a prospect which is rarer than we might fear) or when the kidney is implanted in someone on the cadaver waiting list. This becomes more important as people become harder to match.
Were you able to break the simultaneity constraint, outcomes would be substantially improved. If you put recipients whose donor donated a kidney at the top of the queue for inclusion in any future pairings, you could (at least in France) increase the match rate from below 40% to 63%, and reduce the average waiting time by 50 days. But alas, that is not allowed.
There is one big thing for us to do to improve living donor transplantation. There are multiple donor exchanges, which are all largely siloed from each other. Many donations are arranged locally by the hospitals themselves, who do not pass on the information to others. We end up matching too many O’s to AB’s, when they could be used to start a larger, useful cycle. Agarwal, Ashlagi, Azevedo, Featherstone, and Karaduman (2019) estimate that forcing hospitals to share donors to the central exchange would increase transplants by somewhere between 240 and 500 a year.
We can also improve the allocation of deceased donor kidneys. Unlike with living donors, the surgery cannot be scheduled in advance. Someone must be made an offer, decide whether to take it, and do the surgery at the drop of a hat. These offers must be made sequentially – since we don’t have money, and these are not repeated transactions, we cannot use auction mechanisms like Feeding America used for food banks. The combination of sequential offers, plus kidneys degrading in quality over time, means that we cannot guarantee that every kidney gets used, nor that they will be allocated to the best person.
Finding a better way to order the offers of kidneys is what Agarwal, Ashlagi, Rees, Somaini, and Waldinger (2021) set out to do. They have data from New York City and environs, with around 5,000 people on the waiting list. 1,400 people join the list every year, while only 200 cadaver kidneys are recovered. The list is in a steady state only because people are dying before they can get a transplant.
Both the old and new system ranked the patients with points for tissue-type similarity, being a pediatric patient, how hard they would be to match, and importantly, waiting time. This element of waiting time encourages patients to refuse the offer they are given, because they will expect to receive further, possibly better, offers in the future. The mechanism that reduces wastage would be to make it first come, last served, but as we shall see, this is not actually the best.
It is not enough to simply simulate, given the current observed choices, what would happen under a different mechanism. People are strategic and respond to incentives. Instead, we must estimate the demand for kidneys, which they do using a conditional choice probability model in continuous time.
Conditional choice probability estimation usually resides in discrete time. You have a finite number of states, which are simply combinations of variables, and you observe the choices of each person in each state, plus the probability of transitioning forward to any given state. You can therefore estimate the expected value of being in a particular state by simulating forward many times. Discrete time requires you to pick how long the period length is, as well as figure out what happens when multiple kidneys, so instead they operate in continuous time.
With the estimates of consumer demand, we can try out different policies. If we try out the first come, last served policy, we see that it would reduce the fraction of kidneys discarded by a quarter, but create such a mismatch between patients and kidney characteristics that welfare goes down by the equivalent of a 55% decrease in the arrival rate of kidneys.
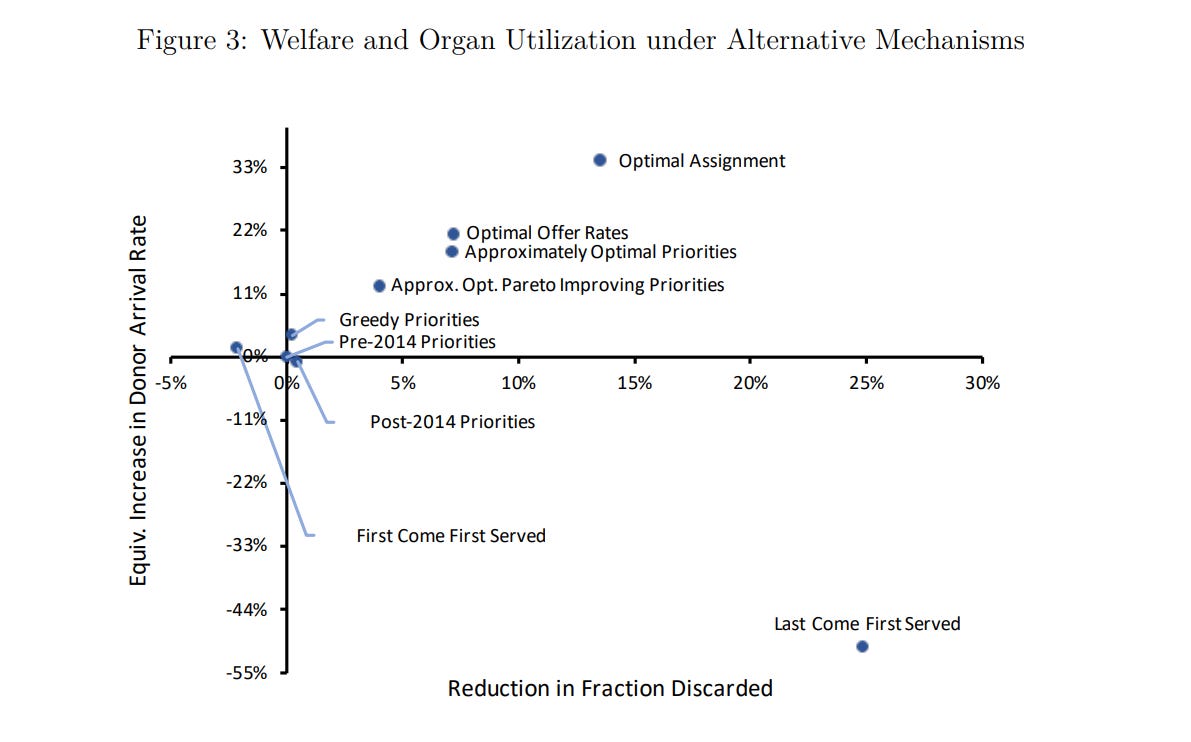
If you knew each person’s preferences, then you could raise welfare by the equivalent of a 33% increase in the arrival rate of kidneys, while reducing wastage by 14%. (Note that you don’t actually want to reduce wastage by 100% – not every kidney from a dead person is worth implanting, even with the enormous backlog). The optimal one which can be reasonably implemented creates an increase in welfare that is equivalent to an 18% increase in the arrival rate.
Unfortunately, the recommendations do not appear to have been adopted. Perhaps they were too complicated – they cannot be summed up as a set of simple rules, but are more of an estimation technique for getting rules specific to a market – but it is only with difficulty that economists can get their recommendations adopted.
This is one thing which bugs me about kidney donation. It is excellent that we have tools for better allocating the kidneys that we do have. It is good to do good things. The only reason we have to be so concerned with allocation, though, is that we have chosen not to do the best thing. The problem is that there are not enough to go around. If we could incentivize people to donate their kidney through money, we would have a lot more kidneys! The magnitude of this dwarfs the possible gains from better systems. Consider the paper on cadaveric donations in New York. An 18% increase in the arrival rate of kidneys is only an increase of 36 kidneys more a year. That’s a big deal for the 36 people who get them – but there are 5,000 people on the wait list!
This is a general problem with mechanism design. The solution is generally just prices. Mechanism design is often useful only when, for no particularly good reason, we choose not to use the best mechanism. We can do a lot of work trying to solve the problem of double coincidence of wants in a barter market, or we can use the tool we invented in ages immemorial for exactly this purpose. The original uses of the trading cycles were for exchanging housing in communist Moscow – why are we trying to do communism marginally better when we could just not do communism at all?
The best examples of useful mechanism design where the problem is not one that we created for ourselves are in allocating resources for the first time. Because of asymmetric information, we cannot simply give out the resources and expect them to be reallocated to the right uses. The initial auction mechanism matters, especially when the simplified assumptions for simple auctions are broken and we need to take into account people having valuations for multiple goods, risk aversion, and other complications. The FCC spectrum auctions are beautiful to me for this reason.
Al Roth would argue that repugnance is just as real a constraint as asymmetric information. I don’t really like this. It seems too conciliatory to the anti-market savages. But if we must live in an imperfect world, there is nevertheless something which you can do. You can donate your kidney. The National Kidney Foundation is, to my knowledge, the best place to do this. I would like to personally encourage you to sign up.
I went through the screening process in the spring of 2023. It was not unpleasant – I collected a large jug of urine, gave a lot of blood for testing, and had a long morning in the Georgetown University Hospital system. Unfortunately, I cannot speak to the experience of actually undergoing the surgery, because I was rejected. (In fact, I learned that I was just on the border of having pre-diabetes, and that I was at risk of kidney failure in the future).
I feel embarrassed to tell others this! I fear that people will think that I chickened out. I did not! They just didn’t want me.
I don’t know what the right way to sell donating a kidney is. All I can give are the facts – it will create a lot of consumer surplus. You won’t capture it, but it is nevertheless good to create consumer surplus. So sign up today!
I'll contribute that I've lived unimpeded in any respect with one kidney from age 58 to (so far) 84.
I started the process too, but then had a (complete surprise) heart attack. After that they wouldn't let me continue. Apparently going down to one kidney puts strain on the heart. Not a problem really, an excess of caution on their part I think. Although I do have an inflammation-prone physiology, chronically elevated levels of eosinophils.